





Let's start by getting one thing straight, right off the bat. The topic of co-sleeping in Australia, and in many western countries for that matter, is controversial. But that doesn't mean we shouldn't talk about it. Far from it, we should embrace healthy conversations about what it means to co sleep and to bed share safely. And yes, some research does show (and some medical professionals believe), it is possible to safely do so with the right tools and information.
There is nothing illegal about sleeping with your baby—whether co-sleeping or bed sharing. You do not need to feel shame about wanting to sleep with this beautiful, perfect human that you created.
If you've ever been a parent to a newborn before (0-3 months old), you have probably experienced the scenario where your little one is sleeping in their bassinet beside your bed, and they're grunting and turning around and generally being a noisy little gremlin. Then, you take them in your arms and suddenly, they're quiet as a mouse. They're peaceful. This is because their bodies are still learning how to regulate their own temperature, their own breathing and their body's homeostasis. They need an adult body to help them do this, and this is what humans have done for their babies throughout our evolution.
And then there's co sleeping. On the one hand, we have devastatingly tired parents, who could fall asleep on a couch with their newborn, and on the other, we have maternal child health nurses who won't share information around how to set up co sleeping arrangements safely.
The unfortunate thing about the fear that has been put into most Australian parents, is that if they do decide they want to co-sleep or sleep bedsharing, they often don't have access to information around a safe sleep environment from the very professionals who are trying to ensure safe infant sleep. So let's shift the narrative, shall we?

Babies generally sleep better with their parents
Because many parents observe that their baby sleeps better with them, at some point they'll explore what co sleeping or bed sharing might look like for their family. So let's start by covering off some of the basics, because there are lots of words that get thrown around and some nuances to these definitions.
What is co sleeping?
Co sleeping is a general term that is used to describe any form of co sleep arrangement between a parent and their child, whether bed sharing, breastsleeping or room sharing. Some forms of co sleeping have been found to have higher risk of sudden infant death syndrome than others and below we'll be diving in to what these are, and how you can still experience the benefits of co sleeping while making sure you get a good night's sleep too.
What is room sharing?
This is a type of co sleeping that is most encouraged by health professionals. This is where, for the first six months of life, it is recommended that a baby sleep in the same room as their parents, in a basinett beside adult beds.
What is bed sharing?
This is a type of co sleeping that is discouraged by most western health professionals. It is the dominant form of sleeping arrangement that humans across history have practiced, and remains the dominant sleeping arrangement in countries such as Japan, Sweden and the Philippines (and Japan has one of the lowest rates of SIDS in the world).
Now, it's important to note that these countries have a number of factors that assist in making bed sharing safe for infant sleep because it is a normal practice there, and we'll cover all of these here. So in its safe form, bed sharing it is where an infant will co sleep on an adult bed with a number of protective and safety factors that reduce the risk of sudden infant death syndrome (or do not increase it).

What is Breastsleeping?
Breastsleeping is a relatively new term, coined in 2015 by Dr James McKenna and his colleague Dr Lee Gettler who are long term researchers and advocates for safe bed sharing, primarily in the context of breastfed babies. It is used to describe the way breastfeeding and bed sharing mutually reinforce one another in a positive way.
Weighing in on the co sleeping controversy that seems to be prevalent in western cultures, this concept is based on research which shows that human infants are biologically adapted to sleep in close proximity to their mothers, and that breastfeeding and bed-sharing facilitate optimal physiological and psychological outcomes for both mother and infant. It has many benefits beyond just the reduction of risk of sudden infant death including:
-
Making it easier for mothers to establish and maintain exclusive breastfeeding for the first six months of their child's life
-
Supporting child health, including the infant's immune system, brain and emotional regulation (all benefits of breastfeeding itself)
-
Improving maternal sleep and well being
I spent some time when my bub was a newborn, reading Dr McKenna's book on co sleeping. It's what helped me feel confident to apply the approaches to my own family sleep environment.
Dr. McKenna's guidance on practicing breastsleeping safely in a parent's bed, is based on his extensive research and clinical experience. His recommendations follow all of the Red Nose and actually go a step further in suggesting that the safest form of bed sharing should be done with breastfeeding at the same time.
In the sections below, we'll detail exactly how to safely set up different co sleeping arrangements for you and your beautiful bub.
How can I room share safely?
Room sharing has been found to be a protective factor in reducing the risk of sudden infant death syndrome. To room share safely, you can:
-
Buy a bassinet
If you'd like to be closer to your baby there are some options that. This is the one we bought for our babe. -
Put it next to your bed
And in cases where you want to attach the bassinet to your bed, the same guidance as bedsharing applies—other than needing the bed to be on the floor. So you should also make sure the primary or breastfeeding parent is the one who sleeps closest to the connected bassinet. -
Do this for the first 6 months of your baby's life and ideally up to a year
If parents prefer, they can then move them to a separate room at this point. Practically speaking, many parents I've spoken to tend to move the baby at 6 months because they need a break from all the weird noises, and find that unless you're bed sharing, both parties sleep better on their own when they're not waking each other up through the night. Lots of this will ultimately depend on your baby's sleeping and feeding patterns, as well as your preferences as a parent in terms of the exact timing. In our case, we did this for 6 months, and then I moved to the nursery and did bed sharing there.

How can I bed share safely?
It's important to note that some health professionals believe that there is no such thing as safe bed sharing. But this is ultimately a value judgement. Consider this: is it safer for you to accidentally fall asleep while feeding or settling your child on the armchair or couch? Or is it safer to get a safe bed sharing environment set up, so that when you are inevitably so tired you cannot even think straight, you'll have confidence that sleeping with your baby is being done in safest way possible? The human biological drive to sleep is so strong, and so disrupted in the newborn phase, that being prepared for this possibility (or even inevitability) is important for new parents.
And we shouldn't forget that many parents choose to co sleep because they want to be physically close with their baby. This is just as valid a reason for wishing to bed share. So, these are the best recommendations for safely co sleeping with your baby that take into consideration known risk factors. These are inclusive of:
-
Red Nose best practice guidelines on bed sharing
-
Further research guidelines available (direct from research papers)
-
Dr Mc Kenna's best practice guidelines on the safest forms of bed sharing
-
If you have a mattress that's soft underneath, get a firm one
Make sure that you're using a firm mattress, one where the sleeping surface is similar to that of a cot mattress. Do not use water beds or air mattresses. We used an Ikea mattress like this with slats directly on the floor and put it in the nursery. -
Set the room up with the mattress on the floor, away from the walls.
This might sound like a lot to do, since most of us in Australia are used to sleeping up on a bed frame, but this is the safest way to co sleep with your baby. And not being worried about them falling off the bed, or having pillows become hazards (which you may use to prevent them falling off), is the safest way to do this. You want to keep the mattress away from the wall, ideally in the middle of the room. This is because having it near or up against the wall can create a scenario where a baby's head gets trapped in between the bed and the wall. This has sadly been the cause of infant deaths before.
*Note I am not going to place links to these stories here because I believe they're too traumatic to read but you're welcome to search and read them for yourselves.
In my case, the first three months we did room sharing with the bassinet attached to our bed, and then once bub could roll, he shared more in our adult bed, but with the bassinet still attached, and once he was six months old, I moved into the nursery with him. This was the best option for us as a family.
-
Keep any adult bedding including loose bedding such as doonas, sheets and pillows, away from the baby
Practically speaking, this means it's usually best (and easiest) to not sleep with a doona or pillow yourself, either. It'll just help you sleep better knowing that you don't have to worry about it! You'll be surprised comfortable this becomes.
-
Preferably, only choose to bed share if you have also breastfed your baby during the first 90 days of their life
Breastfeeding, and in particular breastsleeping (where you simply feed your baby as needed from the breast as they wake throughout the night), confers a protective benefit against SIDS. That means it's something you can do to reduce the risk of SIDS, and it also makes maternal sleep far easier and contributes to their mental health.
-
I personally found that it took a few weeks for me to even be able to learn how to latch my baby in the lying down position properly and even then, for a number of weeks after that, he would still fall off a fair bit. But as noted, the research suggests the breastfeeding benefit isn't limited to breastsleeping, it is anyone who has breastfed their baby (no matter how much) in the first 90 days post birth. That being said, there is further benefits that can be gained from breastsleeping.
As a baby grows, they will improve their ability to snuggle in to you and make it easier to breastfeed on your side while sleeping. Everyone's breastfeeding journey is different and you can learn more about it here, but know that it's quite normal for the lying down position to be a more difficult feeding position to master at first, it just takes practice and time.
-
Place your baby to sleep on their back (not their stomach or their side)
This is the same as guidance for when your baby is in a bassinet or cot too: no bumpers, blankets, toys or items in there and you should purchase one that conforms to the Australian safety guidelines. -
Put them in a safe sleep sack, and never have them swaddled or arms contained
It's important to realise that safe, in this instance, is different to what is safe in a bassinet. It is never considered safe to wrap a baby who is sharing your bed. So use a sleep sack that keeps their arms free and their neck free. Use something like this for summer (or this for those really hot nights) and like this for winter. Do NOT clip or zip up the sides on the newborn version when your baby is in bed with you. -
Don't let anyone else sleep on the bed, other than your co parent
Make sure there aren't other children, pets or adults (who are not the child's parents) in the bed at the same time there is a baby sleeping there. Another sleeping adult or child who fall asleep where an infant sleeps, can effectively become the same kinds of hazards as bed covers and can cause overheating or suffocation.If someone else IS sleeping in the bed with you, make sure that the primary parent or breastfeeding parent is the one who is closest to the baby. Never put the baby in between two adults. Obviously for co sleeping once your infant is over 12 months this is generally not a problem, it's the early days that we're talking about here.
-
Never leave your baby unattended on the sleep surface.
This specifically related to where the mattress of the shared sleep surface is not on the floor. If you have a mattress that is away from the walls and on the floor or carpet, this is of course safer than a bed (especially if your baby can already roll). Australian authorities on SIDS would always recommend that during the day, however, a baby should sleep wherever you're located, in a bassinet. A baby carrier, when worn safely, is also a great option for during the day, but it is best not use a baby carrier while you and your baby are both sleeping. -
Remove any jewellery and tie up your hair
Basically anything that is on your person that your baby could accidentally become tangled in. As horrible as it sounds, there have in fact been cases of infant deaths as a result of accidental hair strangulation. As someone with very long hair myself, this was something I have always taken to heart and made sure my hair was always tied back when I slept with my bub in the first six months!
What are the real risks of sudden infant death syndrome (SIDS)?
SIDS is when a baby who is younger than one year old dies suddenly and unexpectedly during sleep, and no one can find out why even after a careful investigation. The risk of SIDS comes from a number of environmental factors that are related to a parent's lifestyle choices, room set up choices, and the general health and genetic predisposition of the baby which can also be influenced by the mother's environmental choices or circumstances during pregnancy..

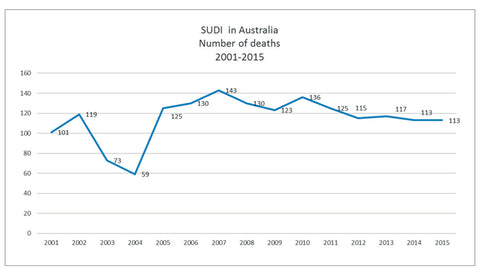
What are the death statistics and risk factors
Public health campaigns have helped to lower the number of SIDS deaths by 50% since the 1990's, educating parents about how to avoid risk factors such as putting babies to sleep on their backs, avoiding smoking around babies, and preventing overheating. The highest risk of SIDS occurs between 2 and 4 months of age. Four months is around about when most babies begin to be able to roll and move themselves better. It is also when they have adapted better to breathing outside of the womb.
In 2020 (the last data on this, although this article was written in 2023), there were 25 known deaths from SIDS in Australia. Another way of putting this, is one death approximately every fortnight. SIDS accounts for 3% of all infant deaths in Australia. There were 11 deaths in Queensland (from 59,490 births), 12 in Victoria (from 75,870 births) and 2 in New South Wales (from 92,541 births). No data is available on deaths from other Australian states. This means the odds of a SIDS death per Australian state is as follows:
-
Victoria - 0.015% - 1 in every 6,322 babies
-
New South Wales - 0.002% - 1 in every 42,270 babies
-
Queensland - 0.018% - 1 in every 5,408 babies
You might wonder why NSW is far lower and I wondered this too, but when I looked at the data and compared total deaths - both SIDS and SUDI together, all the states had similar statistics. So it seems NSW categorises their SIDS deaths differently, and in some cases where VIC or QLD would categorise the death as SIDS, NSW categorises them SUDI deaths.
It is important to note there are other types of infant or gestational deaths that can sometimes be reported at the same time, but they are not SIDS. These include:
-
Neonatal deaths: deaths that occur within the first 0-28 days of life
-
Still birth: deaths that occur between 20 weeks and and may also include late term abortion
-
SUDI: when there is a sudden, unexpected death of a baby and no one knows why. SUDI can include deaths from SIDS, which is when a baby dies during sleep, or from other causes like drowning.
Genetic pre-disposition
For a very long time the cause or the ability to determine individual risk of SIDS hasn't been possible. In 2022, however, there was a breakthrough. Butyrylcholinesterase (BChE) has now been discovered as the first biochemical marker (both genetic and epigenetic), that could help detect babies more at risk of Sudden Infant Death Syndrome (SIDS) while they are alive. Lower levels mean a higher risk of suffering SIDS. While there is no test that you can take to determine the risk of your baby at this time, it is likely something like this will become available over the next decade.
Environmental factors
-
Babies who sleep on their stomach or are placed down to sleep on their side
Because they can then move to their stomach without being used to it - this is in fact found to have greater risk than being purposefully placed on the stomach. -
Parents who smoke, drink or take drugs
This refers to both mothers or fathers, but especially mothers because some of this risk is passed on during gestation, and then after birth. If someone in the bed smokes, drinks or takes drugs then co sleeping increases the risk of SIDS in this case. A completely smoke free environment is best to lower risk for babies. -
Any soft or cushioned sleep surface
In particular, this refers to co sleep that occurs on sofas, couches and armchairs. -
Soft bedding
Things like pillows, blankets, sheepskins, bumper pads, positioners and stuffed animals can increase the risk of SIDS, no matter how they sleep--and even more so if they do so on their stomachs. Babies are safer without blankets. If parents worry about their babies being cold, they can use a sleep sack, or wearable blanket instead of blankets.

-
Head covering and overheating
One study found that more SIDS babies had bedding over their heads than normal babies in their last sleep before death. Infant or adult bedding like doonas, blankets, and quilts can block the baby’s breathing if they cover the head or face. -
Prematurity or preterm infants
Studies have found that babies who are born too early or with a low birth weight are more likely to die from SIDS than babies who are born on time and normal size. This may be because their body systems are not fully developed and they have trouble waking up and breathing well. It is not because they stop breathing sometimes (which is really freaky to hear as a new parent, but is usually normal for newborn babies). -
Bed sharing (sometimes, but not if done safely)
This is defined as sharing the same sleep surface as the baby. Recommendations around this differ because most of the studies are limited by sample size.
An analysis of data from two English studies, with 400 SIDS infants and 1,386 controls, found that:-
Bed sharing or sharing the family bed with a smoker or adult who'd drunk alcohol (2+ units), or was a smoker meant an increased SIDS risk BUT
-
Bed sharing with an adult who was a non-smoker and had not recently consumed alcohol were not at increased risk for SIDS
-
There are a number of factors that can help to identify when a baby may be more likely to have the genetic pre-disposition to SIDS.
Pregnancy risk factors for sids include
-
Getting inadequate or late prenatal care
-
Smoking during pregnancy or being exposed to second-hand smoke
-
Using alcohol or drugs during pregnancy
-
Having a low weight gain during pregnancy
-
Being under 20 years old when pregnant
-
Having anemia or infections such as sexually transmitted diseases or urinary tract infections
-
Having an abnormal placenta
If you had one or more of this criteria when pregnant, the guidance, including from Dr McKenna who is a breastsleeping and bedsharing advocate, to avoid bed sharing.
Protective Factors For Risk of SIDS
Other than things that can increase the risk of SIDS, there are also a range of co sleeping practices that can actually protect against SIDS. These include:
-
Breastfeeding
And the more that the breastfeeding being done is exclusively from the breast (versus pumping or mixed feeding with formula), the more protective it is. A study that looked at eight different groups of people in different countries, including Australia, found that breastfeeding for at least two months can help prevent SIDS, and that it does not matter how much or how often the baby is breastfed. -
Dummy sucking
Dummy (or pacifier) use can also protect against SIDS, but how it works is unknown. It may make babies more alert, control their breathing better, or change their throat shape. The dummy only needs to be in the mouth when falling asleep, not all night. -
Room sharing
As described earlier, this is a co sleeping arrangement where babies sleep near the adult bed, so the parents sleep next to the baby, but not in the same bed. And if this is done for the first six to twelve months of life, it also reduces the risk of SIDS.

From my personal experience, I felt comfortable to bed share with my son from the time he could roll over in our own room with the bassinet still connected to the bed. Then at six months we decided as a family to follow all the safe sleep guidelines for me to co sleep with bub in the nursery. This included getting a hard mattress and putting it on the floor in the nursery, away from the walls. I would also breastsleep (and still do with my now one and a half year old).
If you want to go deep on a more recent perspective on SIDS research and outcomes specific to Australia, this is a great in depth overview (released in 2018).
What information should I trust on co sleeping?
Different countries do have different best practice guidelines. If you live in Australia, according to the Australian Government Department of Health, the National Health and Medical Research Council (NHMRC) is the government agency that provides advice and funding for health and medical research in Australia. The NHMRC develops guidelines based on the best available evidence to assist health professionals, policy makers, and consumers in making informed decisions about health care. The NHMRC also supports the work of Red Nose Australia, which is the leading authority on safe sleeping practices for infants and children in Australia.
It is important to be aware that Red Nose supports a risk minimisation strategy. This means, they will always recommend that it is safest not to bed share and instead, that the baby have their own safe sleep space, on a separate surface, rather than the same surface as you. This is of course their role to do because they must represent all Australians, including those that are at higher risk of being in a situation where their baby may suffer SIDS. They need to create simple, easy to follow guidelines that everyone can follow.
But it is your choice what you decide is the safest option for your baby, and Red Nose Australia acknowledges this too. You can learn more about their guidance specifically around sharing a surface where babies sleep here, and all the best practice guidelines noted in that article (and more) we have covered here.






Leave a comment (all fields required)